







With the growing number of cardiac implantable electronic devices implanted across the globe, the need for transvenous lead extraction (TLE) due to different clinical causes increases [1]. To increase the efficacy and safety of the procedure, the lead-extracting team should be prepared for various unfavourable scenarios, and the facility should be properly equipped for multiple strategy modifications during the extraction. One such case is when the most common extraction strategy via the implant vein proves unsuccessful, or when in the presence of cut or fragmented leads remaining in patients, the extraction via the subclavian route is unsuccessful or even impossible. In those patients, extraction via the femoral vein provides an efficient bailout strategy, which might even be used as a primary access route in some centres [2]. We present a case of a patient in whom such strategy proved efficacious and allowed the extraction of the destined lead after a failed attempt from the implant vein.
A 63-year-old male patient after mechanical mitral valve implantation with tricuspid valve repair and ring annuloplasty, with congestive heart failure due to ischaemic cardiomyopathy was admitted due to lead-related infective endocarditis. The patient had a Biotronik DX implantable cardioverter-defibrillator (ICD) with a floating atrial dipole ring (Figure 1 A), implanted in the secondary prevention of sudden cardiac death 7 years ago. The patient had the device extracted in the setting of the hybrid operating theatre, in the continuous surveillance of a cardiac surgeon. Initially, a locking stylet (Liberator, Beacon, Cook Medical) and compression coil (One-Tie, Cook Medical) were applied. After numerous unsuccessful attempts to advance the various sizes (10F, 11.5F, 13F) of Byrd Dilator Sheaths (Cook Medical) over the lead, the introduction of stainless dilators would also have been unsuccessful (Figure 1 B). Thus, the decision was made to extract the lead using the femoral approach. A Cook femoral Needle’s Eye Snare (13 mm profile diameter) was introduced via the right femoral vein (Figure 1 C), and the lead was successfully captured and extracted through the workstation without any local or systemic complications (Figure 1 D).
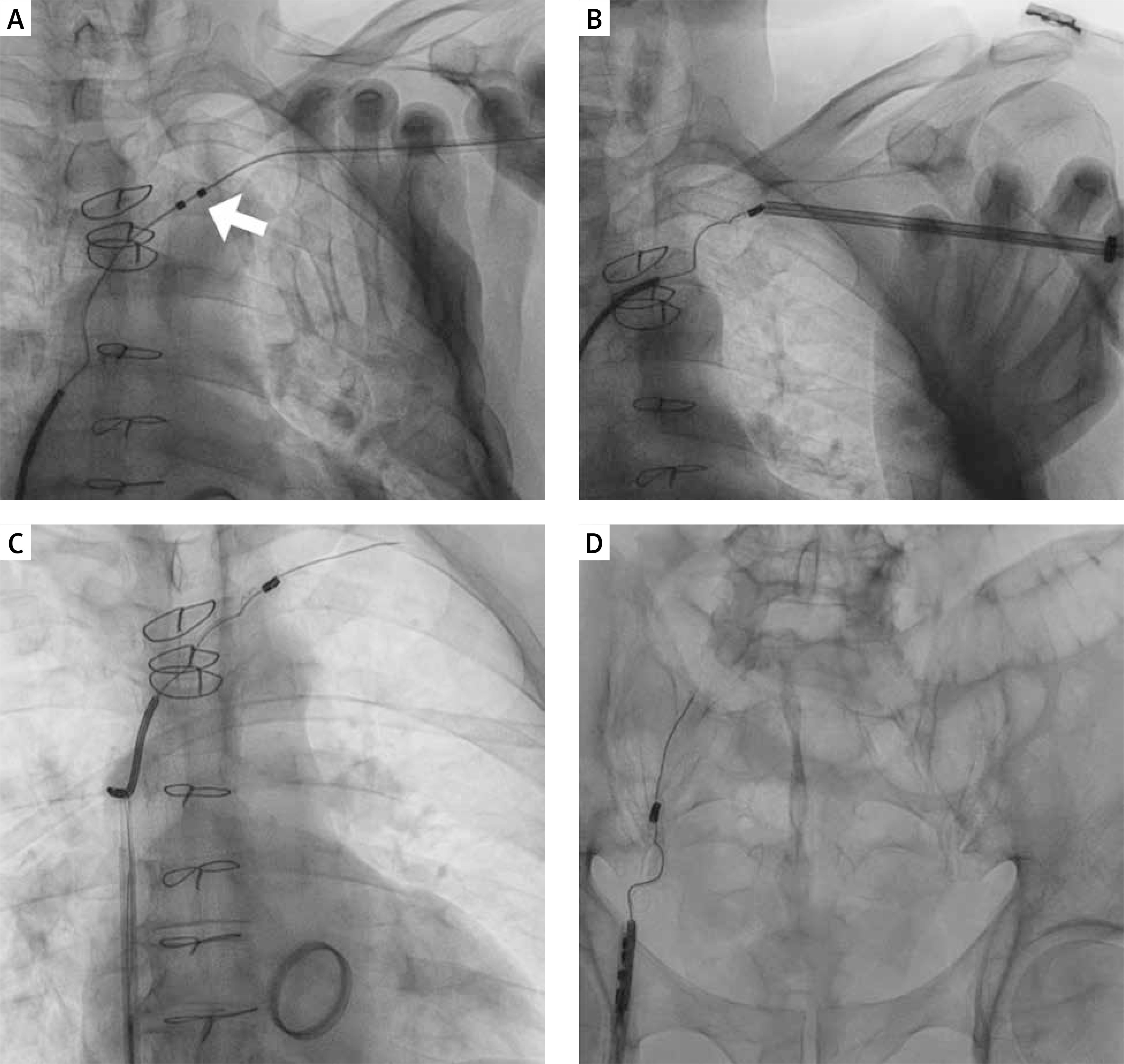
Figure 1
Fluoroscopic images of the described procedure. A – An implanted system with the tip of the lead already extracted into the superior vena cava. An arrow indicates the atrial sensing dipole of the DX lead (Biotronik). B – The consecutive polypropylene and stainless dilators not able to be introduced over the extracted lead. C – The femoral Needle’s Eye Snare (Cook Medical) advances from the right femoral vein, already pictured after successful capture of the right ventricular lead. D – The tip and coil of the lead after entering the workstation seconds before complete extraction from the circulatory system
Our case demonstrates that, for various reasons including the anatomical tightness of the subclavicular region, extraction of the lead via the implant vein might prove ineffective. One of the possible factors decreasing the probability of unobstructed lead extraction is the initial implantation technique. As demonstrated in a recent consensus document on the optimal implantation technique of cardiac devices, the intrathoracic subclavian vein puncture for establishing venous access should not be considered as the first choice because it might increase the risk of mechanical lead-related complications, including the higher risk of lead crush syndrome, in the future [3]. Thus, it can be speculated that in this case, a different initial approach during device implantation could have lowered the risk of the described complications. Nonetheless, in cases similar to the one described or in patients with a fractured lead, modification of the procedural strategy is necessary because further attempts might significantly increase the risk of peri-procedural complications, which have been shown to independently worsen the prognosis after TLE [4]. In such patients, or in subjects with abandoned leads, a femoral snare can prove effective and safe, allowing completion of the procedure.