







Calcified stenosis in saphenous vein grafts (SVG) constitute a challenge in coronary artery disease. The risk for restenosis is clearly higher. High pressure techniques are relatively infrequently used due to risk of calcified graft dissection or perforation with possible cardiac tamponade. In-stent restenosis (ISR) within the underexpanded stent could be a challenge especially if non-compliance balloons (NC) are ineffective. In such a situation intravascular lithotripsy (IVL) using available tools, dedicated to calcified lesions, could be an option [1]. IVL technique uses a balloon-mounted ultrasound source by emitting the sonic energy propagating through the fluid into the calcified vessel wall. Defragmentation of atherosclerotic plaque is an expected aftermath of lithotripsy. Although IVL is not approved in SVG, this kind of off-label treatment could be the only chance for undilatable underexpanded lesions, significantly limiting flow to a relatively large area of myocardium [2].
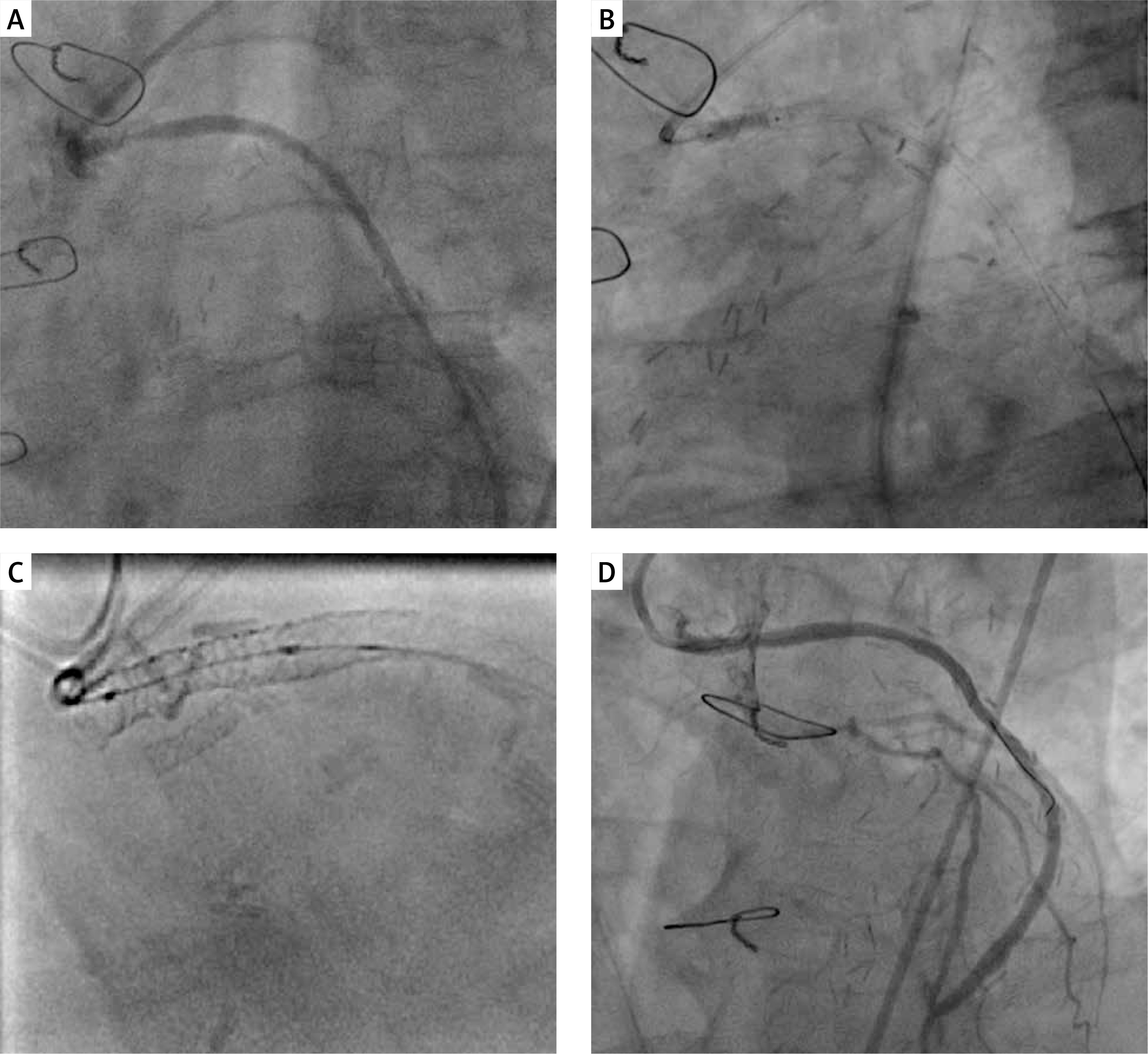
The criteria for off-label treatment by IVL in calcified SVG were met by an 80-year-old man with arterial hypertension, hyperlipidemia, diabetes, after coronary artery bypass graft (CABG) and multiple percutaneous coronary intervention (PCI) of SVG Ao-OM2 treated first with stent implantation in 2015 with follows percutaneous old balloon angioplasty (POBA) drug-coated balloon (DCB) in 2016 and 2019 because of recurrent in-stent restenosis. Even after DCB POBA treatment non-optimal results were achieved and the patient had recurrent effort angina. Due to symptoms of stable CCS class III angina with another critical restenosis in the underexpanded Ao-OM2 SVG stent (Figure 1 A) with critical, long multi-level stenosis in the circumflex and OM2 artery, the patient was qualified for IVL of recurrent ISR on 28.11.2019. After initial predilatation with the NC balloon (3.5 × 15 mm) full expansion was not achieved. The multilevel depths of calcium and the treatment effect assessment were visualized by angio and stentboost technique. The procedure was continued using a 3.5 × 12 mm IVL balloon (Shockwave Medical), which, after completing 80 cycles, allowed for visible better expansion of the balloon at 6 atm (Figure 1 B). The effect was optimized by a 3.5 × 15 mm NC balloon with final inflation of DCB (3.5 × 20 mm 14 atm, 60 s). The final stentboost visualized correct stent expansion (Figure 1 C) with a fully acceptable angiographic result (Figure 1 D). Twenty-one months after the procedure the patient remains in stable condition without symptoms of exercise angina and with no indications for coronary artery catheterization.
Figure 1
A – Critical recurrent stenosis in SVG Ao-OM2 graft. B – 3.5 × 12 mm (6 atm) IVL Shockwave Medical balloon inflation. C – Final stentboost with stent expansion assessment. D – Final angio after 3.5 × 20 mm (14 atm) DCB delivery
The IVL technique is one of the possible tools in heavily calcified lesions. Although the number of IVL procedures is growing rapidly, old SVG is still an off-label indication for lithotripsy. Re-stenting an ISR lesion, old underexpanded stents, growth of neointima, peri-stent calcium deposits, and multiple old stent strut layers are, on the other hand, the most important determinants of possible restenosis. The specificity of degenerated venous bypass angioplasty basically excludes some tools such as ultra-high pressure balloons or rotational atherectomies. In recurrent restenosis in underexpanded stents low pressure technique of IVL may be considered in old, calcified and undilatable changes if the risk of ultra-high pressure technique is unacceptable. A comprehensive approach of preliminary IVL with subsequent NC balloon inflation with final DCB delivery may be an effective solution to achieve an acceptable effect in persistently recurrent SVG ISR.