







Cutaneous leiomyomas are rare benign tumours originating in smooth muscle cells, and account for 5% of all leiomyomas [1]. Piloleiomyomas (PL) arise from the arrector pili muscle [2]. PL may be a single lesion, but more often they are multiple [2, 3]. Dermoscopic patterns usually include delicate pigment network with total distribution [2, 4]. Segmental (zosteriform) distribution was rarely found [3]. Here we present a case report of multiple segmental piloleiomyoma.
A 49-year-old female patient was admitted to the Skin Cancer and Melanoma Outpatient Clinic due to multiple nodules in the skin of the right lumbar region (with a segmental pattern) and the left arm (Figure 1 A). The lesions were tender when exposed to cold temperatures and have been stable since the age of 20. The patient had been diagnosed dermatologically for many years with no clear diagnosis. The patient had hysterectomy without removing adnexa at 40 years of age, due to uterine leiomyomatosis and 6 years later unilateral ovariectomy due to the presence of cysts on the left ovary.
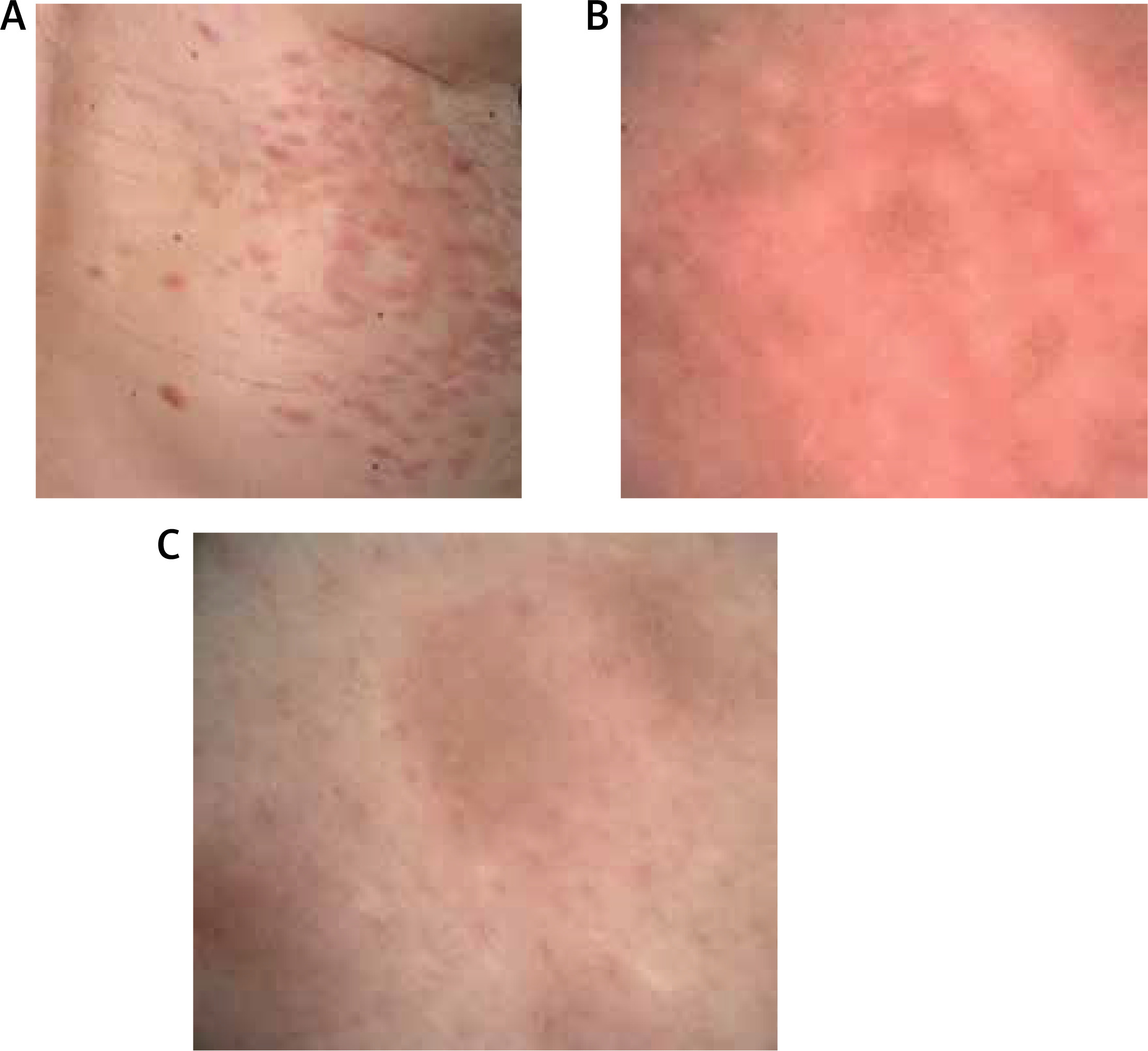
Figure 1
Clinical and dermoscopic examination. A – Clinical examination of the right lumbar region showed the presence of multiple reddish nodules distributed with a segmental distribution. B, C – Dermoscopic examination of the lesions revealed the presence of discrete, reticular brownish lines, mixed with numerous whitish clods of variable size and number throughout the whole lesions (polarized-light dermoscopy, DermLiteFoto dermoscope (3Gen), LLC, San Juan Capistrano, CA, USA, 10× magnification)
The authors have received the approval from the local ethics committee of the National Research Institute of Oncology (reference number KB/430-29/19). The study was conducted in accordance with the Helsinki Declaration of 1964, and its later amendments. All subjects provided informed consent to participate in the study as well as for publication.
Dermoscopy revealed the presence of discrete, reticular brownish lines, mixed with numerous whitish clods of variable size and number throughout the whole lesions (Figures 1 B, C).
A surgical biopsy specimen showed intersecting, well-differentiated smooth muscle bundles composed of spindle cells with elongated nuclei eosinophilic cytoplasm, with no atypia (Figure 2). Some of the cells were enlarged and hyperchromatic, similar to those seen in uterine leiomyomas. The specimen showed smooth muscle actin (SMA) positive expression. Mitotic activity was non-brisk, with Ki67 index of approximately 1%.
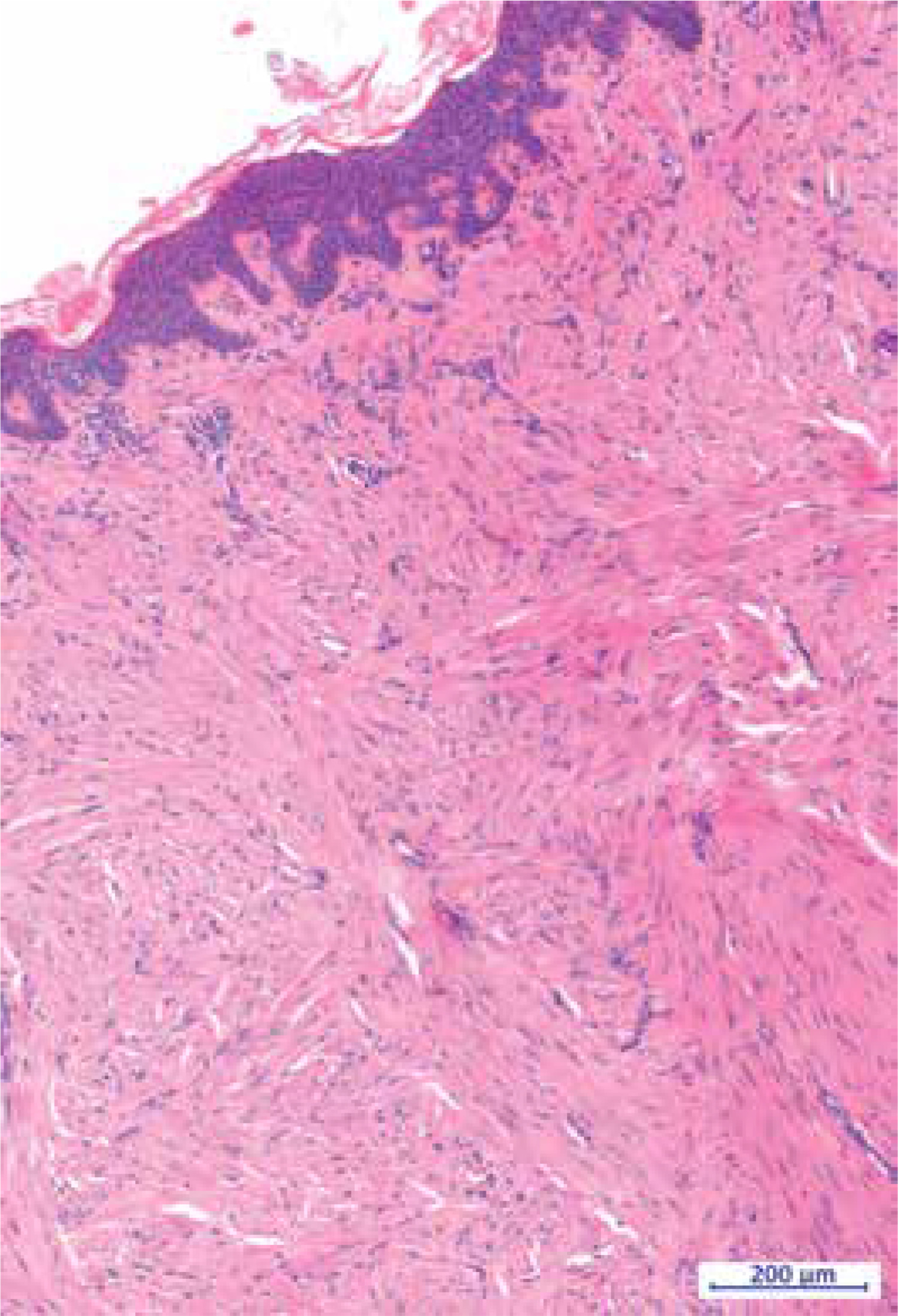
Figure 2
Histopathological examination of the lesion confirmed the diagnosis of piloleiomyoma; intersecting, well-differentiated smooth muscle bundles composed of spindle cells with no atypia, elongated nuclei and eosinophilic cytoplasm. Proliferation seen here is poorly circumscribed. Some of cells are enlarged and hyperchromatic, similar to those seen in uterine leiomyomas (hematoxylin and eosin stain, 7.22× magnification)
The treatment consisted of the surgical excision of the largest nodule, which caused pain and discomfort due to its tenderness. As part of the follow-up, the patient had the ultrasound of the abdomen and right ovary, but no abnormalities were found. The patient remains in dermatological observation.
Multiple piloleiomyomas could be accompanied by uterine leiomyomatosis, or rarely by renal cell carcinoma [3, 5]. Simultaneous incidence of multiple piloleiomyomas and renal cell carcinoma has been described as hereditary leiomyomatosis and renal cell cancer syndrome (HLRCC), which is an autosomal dominant disease [5]. Patients often present with piloleiomyomas which are painful when exposed to cold [5]. Commonly, patients have co-existing uterine leiomyomas, and they require screening for renal cell carcinoma [5]. The pain related to multiple piloleiomyomas can be severe and may be difficult to treat [6].
Dermoscopic patterns described in multiple piloleiomyoma may vary. In the study of 114 histopathologically confirmed cases of PL, most often the lesion had a symmetric, delicate pigment network with multiple hypopigmented areas, without the presence of vascular structures or ulceration [2]. However, lesions located on the head and neck were also reported as papules with discrete brown reticular lines and white clods [3]. In the same patient, lesions on the back revealed brown lines of irregular or parallel distribution [3]. Another study described 2 cases of multiple segmental PL with multiple yellow-to-white clods [7].
Due to its rare occurrence, the diagnosis of PL may be difficult. Early clinical diagnosis supported with dermoscopic examination may be crucial for detection of possible comorbidities at the early stage, including cancer screening.
In conclusion, the characteristic dermoscopic presentation, painful lesions on low temperatures, and segmental arrangement of nodules, as combined elements of the history and physical examination, facilitate the initial clinical diagnosis of piloleiomyoma, and consequently the initiation of appropriate treatment, including surgical treatment in the case of painful lesions, significant size or for best aesthetic-functional reasons.