







Phytophotodermatitis is a phototoxic cutaneous eruption due to skin exposure to furocoumarins, which are organic chemical compounds produced by a variety of plants, and ultraviolet radiation from sunlight. Mild skin lesions can be observed relatively often among children and adolescents [1]. Severe cases (phytophotodermatitis bullosa corresponding to burn injury grade I–II) are rare, mostly occur in adulthood among gardeners and farmers. In certain geographical locations, especially in Europe, Giant Hogweed (Heracleum mantegazzianum) and Sosnowskyi Hogweed (Heracleum sosnowskyi) are particularly implicated in causing such skin lesions [2–4]. Among other inducing factors, citrus fruits (lemons, limes), fig, celeries, parsley, or carrot leaves should be noted [5–10]. Phytophotodermatitis may also be an occupational disease among grounds operatives [11].
In most cases, the diagnosis of phytophotodermatitis can be made after taking a detailed medical history; however, the inducing factor may not be immediately apparent. Mild cases of phytophotodermatitis are self-limited and need only symptomatic management; these patients are usually referred to and treated by dermatologists. However, patients with more severe inflammatory eruptions should be hospitalized and treatment might involve minor surgical interventions, and administration of intravenous steroids and antibiotics [3]. Uncontrolled superinfection may lead to unusual complications with severe consequences [12].
We report the case of an elderly male patient with acute phytophotodermatitis requiring hospitalization due to the severity of local dermal inflammation and the patient’s older age and co-morbidities.
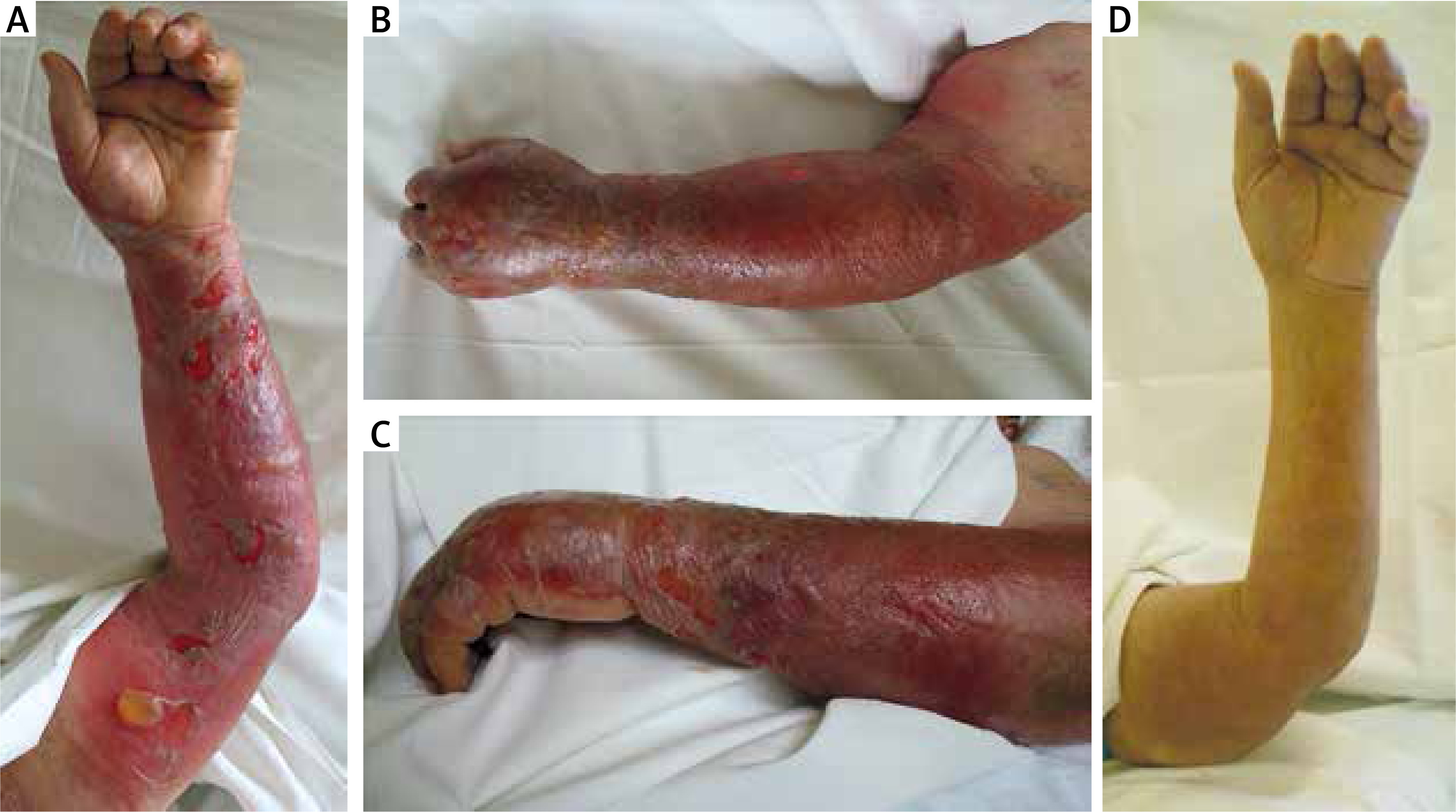
The 83-year-old male patient was admitted to the emergency department with a 2-day history of painful blistering wounds over the entire left lower and upper arm (Figures 1 A–C). Living in a farm, he collected green grass and small plants for his rabbits while working in strong sunshine for hours in June. The patient used his left hand to carry the plants, without clothes covering his arm; and the burning pain and blistering began to develop on the subsequent day. Only the arm was affected, other skin areas were free from sings of dermatitis. The patient experienced chills at home in the morning and was subfebrile some hours later. In the past medical history, type 2 diabetes treated with human insulin four times daily and heart failure stage NYHA II–III due to coronary artery disease were documented; no other precipitating factors or events possibly leading to dermatitis were explored. The patient was referred to our medical department for treatment.
Figure 1
A–C – Marked erythema and blisters on the upper and lower uncovered left arm of the patient on admission (a farmer collecting grass and small plants around his home in summer on the sun, which resulted in development of phytophotodermatitis bullosa on the subsequent day). D – Full recovery after 6 weeks
On admission, C-reactive protein level was high (359 mg/l), the white-blood cell count was elevated (20.0 G/l) while diabetes was well controlled by using insulin. The clinical presentation was characteristic for phytophotodermatitis bullosa. Notably, a relatively sharp margin between the affected and unaffected skin lesion on the upper arm was observed. The patient identified toxic hogweed (Giant or Sosnowskyi) on a picture, corroborating the cause of dermal inflammation on his left arm. Local disinfectants, antibiotics (amoxicillin/clavulanic acid) and short-term methylprednisolone intravenously were applied but the affected blistering skin required minor surgical interventions (debridement, bullectomy, fasciotomy). Clinical signs of heart failure gradually improved mainly due to administration of loop diuretics during hospitalization. After a long (6 weeks) healing period the patient fully recovered (Figure 1 D). The unusually severe manifestation and the subsequent long healing period were probably due to the advanced age of the patient and long exposure time on sunshine but co-morbidities such as type 2 diabetes and heart failure might be also of importance in this respect. Notably, at discharge the patient was advised to avoid direct contact with furocoumarins (i.e. Giant Hogweed and Sosnowskyi Hogweed around his home) in sunlight to prevent recurrences of phytophotodermatitis.
In conclusion, we herein present an unusual case report showing that phytophotodermatitis may lead to severe local inflammation where topical and systemic treatment with antibiotics and steroids in combination with minor surgical intervention finally leads to complete healing. Importantly, our case emphasizes that plants may cause severe phytophotodermatitis mimicking burns. Proper diagnosis, and timely intervention may lead to better outcomes with complete recovery. Of note, phytophotodermatitis is preventable, therefore, public awareness on medical complications of direct skin contact with certain plants on the sun should be raised.