







A 46-year-old woman with resistant hypertension, chronic heart failure, hyperlipidemia, obesity (body mass index (BMI) 30 kg/m2), and hypertensive retinopathy was admitted for percutaneous renal artery denervation (RDN). She experienced severe headaches (10/10 on the NRS scale) and visual disturbances. Five months before admission, central retinal artery occlusion of the left eye occurred. 24-hour ambulatory blood pressure monitoring (ABPM) revealed increased blood pressure (mean value: 191/125 mm Hg; during day 195/130 mm Hg; during night 186/121 mm Hg, non-dipper circadian rhythm) despite using pharmacotherapy with nine antihypertensive drugs: telmisartan (2 × 40 mg), bisoprolol (1 × 5 mg), amlodipine (2 × 10 mg), spironolactone (1 × 25 mg), torasemide (1 × 5 mg), indapamide (1 × 1.5 mg), doxazosin (1 × 4 mg), clonidine (3 × 225 μg), methyldopa (3 × 250 mg). Secondary hypertension causes were excluded. Moreover, she had no symptoms of obstructive sleep apnea.
RDN was performed using the Symplicity Spyral multi-electrode catheter (Medtronic, Minneapolis, MN, USA). Ten ablations of the left renal artery and fourteen ablations of the right renal artery were conducted (Figures 1 A, B). The procedure was uneventful. Post-procedure ABPM showed significant blood pressure reduction (mean value: 146/73 mm Hg, during the day 150/77 mm Hg, during the night 144/70). The patient was discharged with eight antihypertensive drugs: telmisartan (2 × 40 mg), bisoprolol (1 × 5 mg), amlodipine (1 × 10 mg), spironolactone (1 × 25 mg), torasemide (1 × 5 mg), indapamide (1 × 1.5 mg), doxazosin (1 × 4 mg), clonidine (3 × 225 μg).
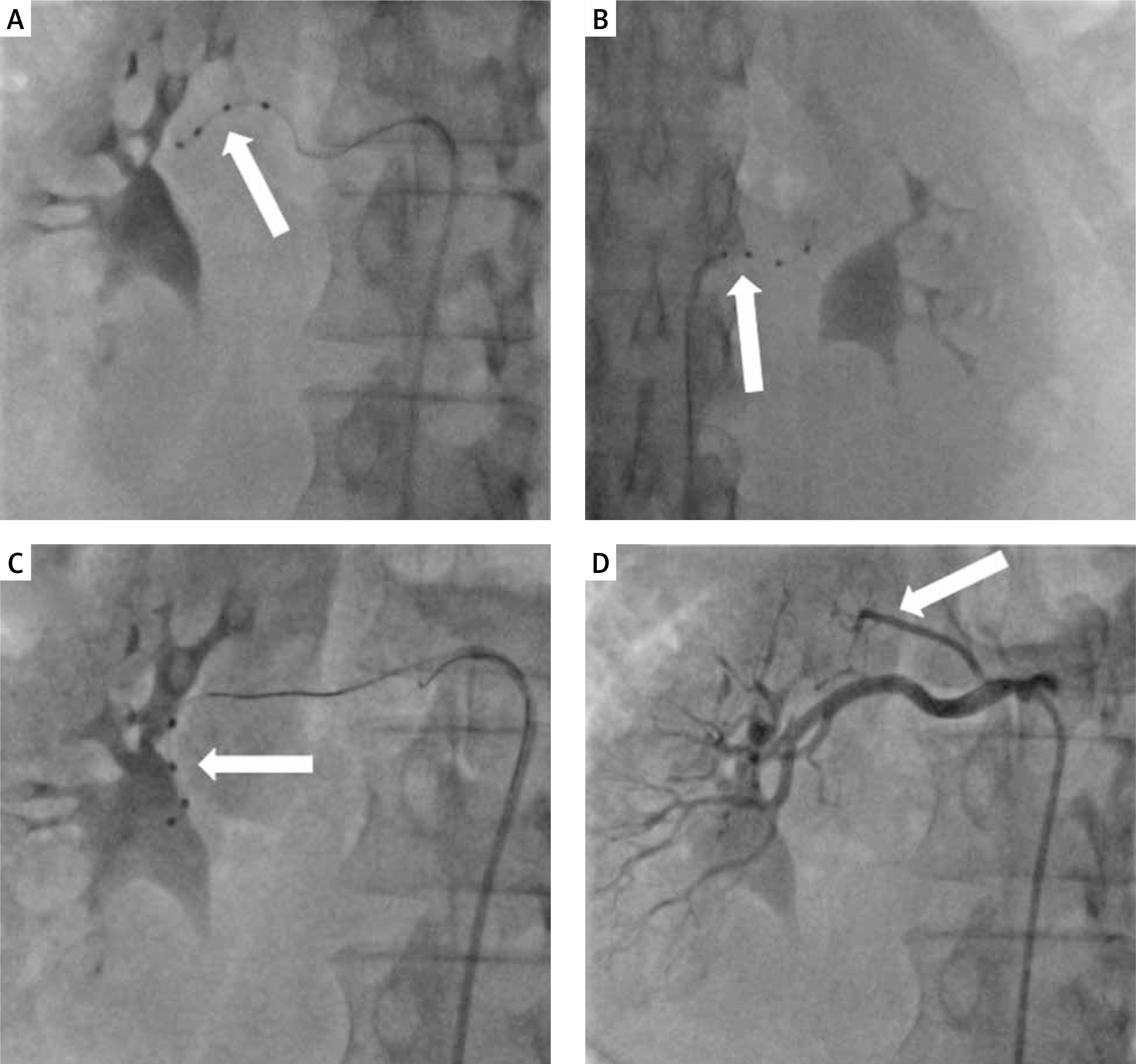
Figure 1
A, B – Initial renal artery denervation procedure (2020) using the Symplicity Spyral catheter in the right and left renal arteries (white arrows). C – Repeat renal artery denervation procedure (2021) using the Symplicity Spyral catheter in the right renal artery (white arrow). D – Right renal artery angiography showing the early polar branch of the right renal artery (white arrow)
Two months later, severe headaches returned, and ABPM revealed high blood pressure (mean value: 188/124 mm Hg, during the day 192/130 mm Hg; during the night 185/119 mm Hg). Hypertension therapy was modified: lisinopril (2 × 40 mg), bisoprolol (1 × 5 mg), amlodipine (1 × 10 mg), spironolactone (1 × 50 mg), torasemide (1 × 5 mg), indapamide (1 × 1.5 mg), doxazosin (1 × 8 mg), clonidine (3 × 225 μg). Due to the persistence of the symptoms and the initial significant decrease in blood pressure after RDN, a repeat procedure was indicated. The RDN procedure was performed using the Symplicity Spyral multi-electrode catheter. Eighteen ablations in the left renal artery and sixteen ablations in the right renal artery were performed during the second procedure (Figure 1 C). Blood pressure decreased significantly (ABPM mean value: 146/78 mm Hg, during the day 147/77 mm Hg; during the night 143/79 mm Hg). The patient was discharged with seven antihypertensive drugs: lisinopril (2 × 40 mg), bisoprolol (1 × 5 mg), amlodipine (1 × 10 mg), spironolactone (1 × 50 mg), torasemide (1 × 10 mg), indapamide (1 × 1.5 mg), doxazosin (1 × 8 mg).
Follow-up visits revealed high blood pressure values again. ABPM performed after one month showed a mean daily blood pressure value of 191/108 mm Hg (during the day 199/114 mm Hg; during night 170/92 mm Hg) and after 6 months: 210/106 mm Hg (during the day 220/112 mm Hg; during night 189/96 mm Hg).
According to the European Society of Cardiology and the European Society of Hypertension (ESC/ESH) guidelines, RDN is not routinely recommended but can be performed in specialized centers in patients in whom multidrug pharmacotherapy of hypertension is ineffective [1, 2].
Accessory renal arteries or early branches of the renal arteries and their incomplete denervation are associated with a lower RDN response rate. Additionally, patients with resistant hypertension have a higher prevalence of accessory renal arteries. Our patient did not have the early polar branch of the renal artery ablated due to its small diameter (Figure 1 D). Most of the clinical trials performed so far have not performed ablation in vessels < 4 mm in diameter [3, 4]. Precise patient selection appears crucial for improving RDN effectiveness [5].