







Herein we describe the case of a 73-year-old woman who was admitted to the Emergency Department early in the morning because she experienced an episode of intense substernal chest pain that started a day before. This pain was intermittently recurring in different intensities until the admission. At the time of examination she still reported chest pain but of significantly lower intensity (3/10). The admission electrocardiogram (ECG) showed sinus rhythm with a heart rate of 80 bpm, normal cardiac axis, and significant ST segment elevation (STE) in anteroseptal leads (V1-V3, Figure 1 A). A diagnosis of acute STE myocardial infarction (STEMI) of the anterior wall was made, the patient was immediately loaded with dual antiplatelet therapy and emergently referred to catheterization laboratory. The coronary angiogram showed a non-dominant right coronary artery (RCA) that was occluded in the proximal segment (Figure 1 B) with no occlusive disease in the left coronary circulation (Figure 1 C). A weak distal retrograde filling of the RCA by the collaterals (Rentrop 1 grade) from the left-dominant coronary system was noted. A successful primary percutaneous coronary intervention (PCI) of the RCA was performed; it consisted of pre-dilatation with MiniTrek semi-compliant balloons (1.5 × 15 mm and 2.0 × 20 mm) followed by the implantation of Orsiro 2.25 × 18 mm drug-eluting stent. The TIMI-3 flow through RCA was restored with no vessel dissection (Figure 1 D). The initial high-sensitivity cardiac troponin T and NT-proBNP levels were 79.5 ng/l (99th percentile upper-reference limit of 14 ng/l, Roche Diagnostics) and 1085 pg/ml, respectively. On the day following the intervention, hs-cTnT levels were measured again and they were 1341 ng/l. Follow-up ECG after PCI showed normal sinus rhythm of 67/min, normal cardiac axis, and resolution of the STE in anterior leads and return of ST segment to baseline. The predischarge transthoracic echocardiogram showed ischemic cardiomyopathy with preserved global left ventricular ejection fraction (62% biplane Simpson), inferior wall hypokinesia, mild right ventricular dysfunction (TAPSE 16 mm and S’ 9 cm/s), and grade I diastolic dysfunction.
Figure 1
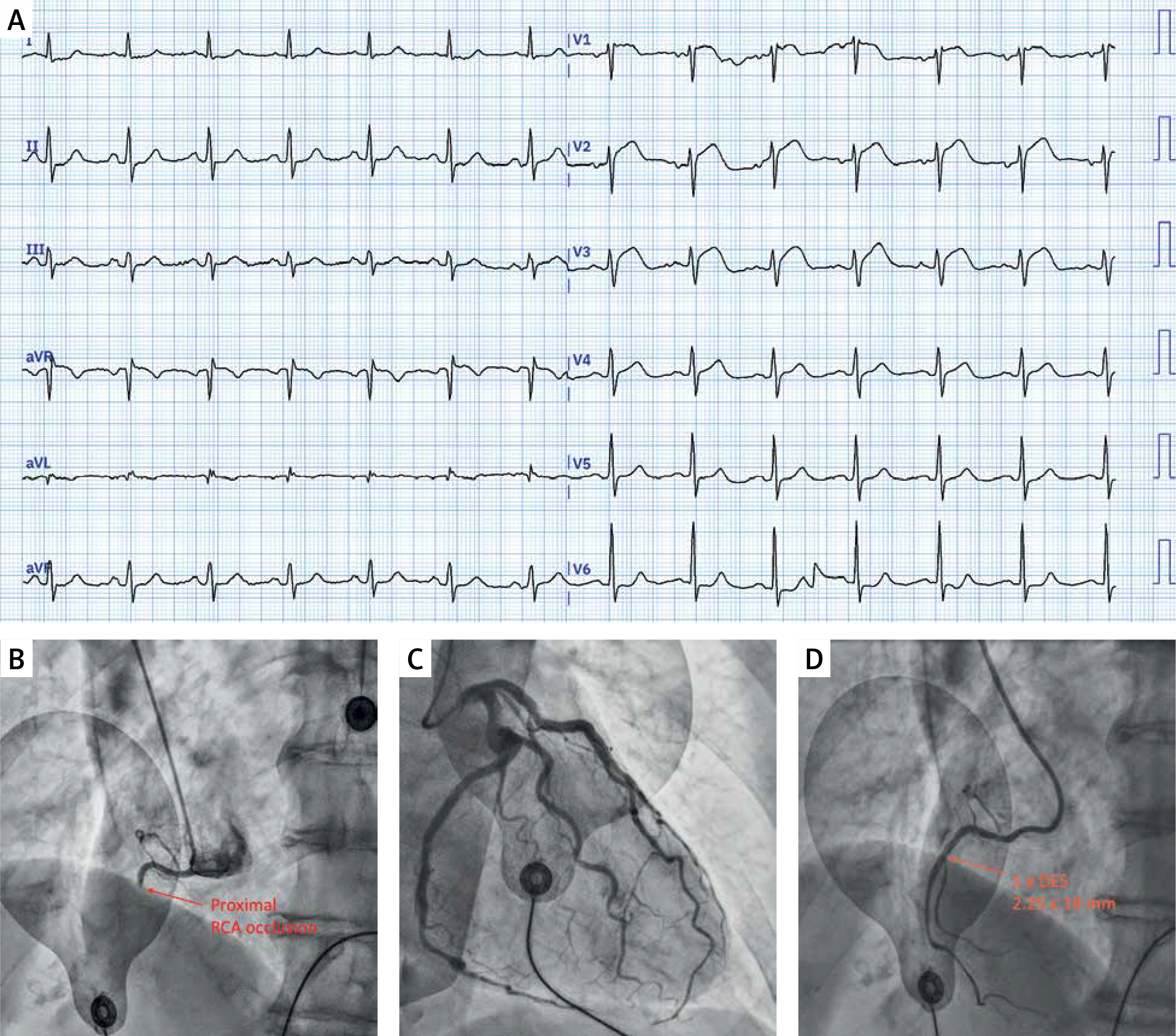
A – A 12-lead admission electrocardiogram showing anterior ST segment elevations in leads V1-V3 with no anterior Q waves and no ischemic changes in inferior leads. B – emergent coronary angiography showing occlusion of the proximal segment of the right coronary artery (RCA) beyond the right ventricular branch. C – selective intubation of the left coronary artery showed left-dominant coronary circulation with no significant coronary artery disease. D – restoration of TIMI-3 flow in the RCA following drug-eluting stent (2.25 × 18 mm) implantation – after reperfusion RCA was revealed as a gracile and non-dominant vessel
This clinical case represents an electrocardiographic and angiographic “mismatch” regarding the culprit vessel responsible for the occlusive MI (OMI), in this case – proximal RCA occlusion with STE in the anterior wall and no pathological changes in the inferior leads. Several learning points and “clues” for this can be derived from the literature and might prove useful for clinicians.
Firstly, when RCA occlusion is proximal to the branch that perfuses RV (right ventricular marginal branch-RVB), STE phenomenon in precordial leads can be observed [1, 2]. Importantly, RCA vs. LAD occlusion can be differentiated as RCA occlusion will typically not be accompanied by developed anterior Q waves while peak STE in anterior leads will occur in V2 with a progressive decrease of STE amplitude towards leads V3-V4 [3]. Furthermore, the finding of a precordial STE in inferior wall STEMI is associated with a smaller infarct size and better left ventricular function [1], especially if RCA is not dominant and does not supply the posterior wall, such as in this case. The presence of distal collateral circulation from the left coronary system perfusing the inferior wall is also associated with precordial STE in inferior STEMI [2] and weak collaterals to distal RCA from left circulation were observed. Finally, proximal occlusion of a small and non-dominant RCA, such as in this case, will not generate significant posterior wall infarction while significant STE will be observed if recording of additional right precordial leads (V3R-V4R) is performed [4]. Finally, findings such as in this case might be present in about 3% of all acute coronary syndrome cases and would most likely occur in the context of an isolated RV infarction with a high proximal obstruction of a small and non-dominant RCA such as exemplified in this case [5].