







Introduction
Atopic dermatitis (AD), also known as atopic eczema, is a chronic pruritic inflammatory skin disease affecting approximately 15% to 20% of children and 1% to 3% of adult population worldwide. AD poses a significant impact on patients’ quality of life (QoL), as well as the QoL of their family members mainly due to disturbance of professional, social, emotional, personal and family life, as well as the presence of various comorbidities. Moreover, AD also causes a financial burden for the patients, their families and healthcare givers [1–6]. The typical onset of disease is the early childhood, and it usually resolves until adulthood; nevertheless, it is estimated that 10–30% of patients will carry on to have symptoms [1]. It has been also shown that adults with AD are prone to work-related aggravation of skin changes with a higher risk of sick leave comparing to the general population [7, 8]. It is clear that establishing disease control has far-reaching importance for patients, their families, healthcare givers and employers. Therapeutic goals and treatment require a combined approach, based on more than one treatment modality, in order to achieve the longest possible period of remission. Disease control could be achieved by administration of topical corticosteroids, topical calcineurin inhibitors, different forms of phototherapy, systemic immunosuppressants and the most recent and innovative therapy – biologics [9–11]. Heliotherapy (HT) in the form of heliomarinotherapy, heliothalassotherapy or climate therapy is a light-based therapy, proven to be convenient for alleviating inflammatory skin changes. The UV lights reach the most outer layers of skin including epidermis and underlying dermis triggering immunosuppression, urging apoptosis, suppressing cellular proliferation and inducing vitamin D production [12, 13]. Furthermore, it is considered that light therapy has strong antipruritic effects, being able to reduce the most disturbing symptoms of AD [14]. The ability of HT to ameliorate disease severity in patients with psoriasis is fairly-well researched, enabling HT to be a well-established treatment option during summer months for the patients in Nordic countries. Contrary to that, the efficacy of HT in AD is sparsely described in the literature [15].
Aim
The objective of this study is to assess the ability of individual HT to ameliorate disease severity and improve the QoL in patients with atopic eczema in the shorter (immediately after HT) and longer terms (3 months after HT). We expect that the immediate effects of HT are fulfilling, taking into consideration all the benefits that HT has on skin inflammation. On the other hand, the long-term ability of light therapy to improve the QoL and skin changes has revealed uncertain results so far and moreover there is no sufficient number of studies scrutinizing this topic. Additionally, as far as we were able to observe, there were no studies examining the effects of individual HT in the scientific databases. Thus, the emphasis of the study is to evaluate the ability of HT to reduce SCORAD and EASI indices, DLQI and SPS scores particularly in the long term, as well as to correlate the obtained results with the outcomes of existing studies.
To our knowledge, studies examining the effectiveness of HT in patients with atopic eczema have not been conducted either in Montenegro or in the surrounding countries so far.
Material and methods
Study design and setting
The study aims to appraise the efficacy of HT in improving disease activity, QoL and reducing pruritus intensity in patients with AD living in Montenegro. The patients with moderate to severe forms of AD were exposed continuously to natural UV lights 3 to 4 h daily (2 h in the morning and 1/2 h in the afternoon), avoiding the hours of the highest radiation and usage of sunscreens. All of the patients pursued 2-week HT during July or August 2021, at the Montenegrin coast. It is estimated that Montenegro has an average of 270 sunshine hours during summer months [16]. Before the HT, patients were informed in detail about the plan and goals of the therapy, as well as its side effects. It was pointed out that if any adverse effects occur, patients should immediately cease the therapy and report to the emergency medical service. All of the observed patients had an appointment for the evaluation with the same dermatologist at the Clinic of Dermatology, Clinical Center of Montenegro, 1 to 2 days before commencing HT (Time 1/T1), then 1 to 2 days right after HT (Time 2/T2), and 3 months after HT (Time 3/T3). The study approval was obtained from the Ethics Committee of the Clinical Center of Montenegro (no. 03/01-9174/1).
Eligibility criteria
The patients included in the study are long-term patients, who have summer homes at the seaside of the country, where they regularly spend summer holidays, but do not live there. All of them were sunbathing on a voluntary basis and according to their holiday schedule. Further inclusion criteria were satisfactory compliance with the previous therapy, willingness to follow and obey the sunbathing plans, cooperate with the assigned dermatologist and show up at follow-up checks at the designated appointment time. Exclusion criteria were Fitzpatrick’s skin photo-type I, past or present malignancies, uncontrolled comorbidities, photosensitivity, family history of malignant skin diseases, any other chronic inflammatory skin disease (i.e. psoriasis, etc.), lack of compliance with the previous therapy, excessive alcohol consumption, and drug usage.
Methods of assessment
Disease severity/activity/extent were evaluated using two validated clinical indices that are related to each other, but have notable differences as well. SCORAD index (SCORing Atopic Dermatitis) is a standardized tool, with a value ranging from 0 to 103, and includes 6 signs (erythema, excoriation, oedema/papulation, crusting, lichenification and dry skin for a representative area in eight body sites), as well as two subjective criteria, sleeplessness and pruritus [17]. EASI (The Eczema Area and Severity Index) is a tool that assesses only inflamed area (erythema, excoriation, papulation/induration, lichenification in four body sites), not including a grade for dryness and scaling. The EASI score comprises the range from 0 to 72. The lower the score, the better improvement in disease activity is achieved [18, 19]. For assessing the impact of AD on QoL at three times, we used DLQI (Dermatology Life Quality Index) questionnaire, authorized and validated for patients aged 16 and above. The higher the score, the more QoL is impaired [20, 21]. SPS (Severity of Pruritus Scale), a four-point score from 0 (no itching) to 3 (bothersome itching/scratching that disturbs sleep), was used to measure pruritus intensity [22]. Finally, we collected the values of UV indices for each patient and every day separately, calculating the mean UV index for each patient for a total of 14 days.
Statistical analysis
Descriptive analyses were used for examining mean, range, percentage values, SD (standard deviation) of different categories. The Wilcoxon signed-rank test was used for comparing the values of scores at three times. A one-way repeated measure, also known as a within-subjects ANOVA, is used to assess assigned scores at multiple times. The χ2 test and the Fisher exact tests were used for analysing correlations among the variables. A two-tailed probability value of 0.005 or less was considered significant. All statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS, Chicago, IL, USA), version 20.0 for Windows.
Results
Participants
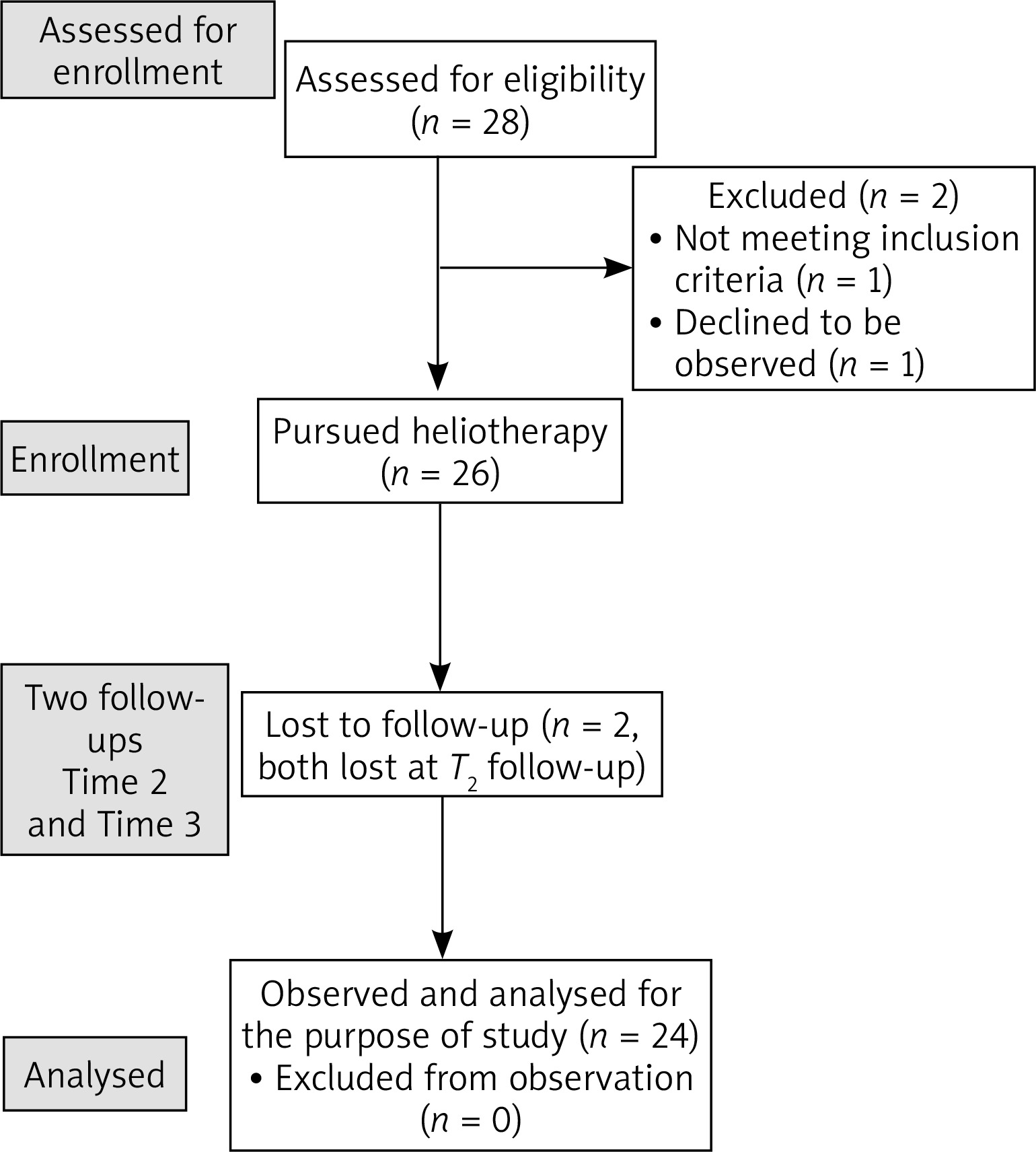
Twenty-six patients were randomized and pursued light therapy. However, two of them failed to appear on their follow-up checks due to job duties and a sudden business trip. Therefore, they were excluded from the analysis. Finally, a total of 24 patients were allocated for the analysis. All of them met criteria for inclusion, were exposed to HT according to the given directives, while obeying and following all the instructions and routinely showing up at the follow-up appointments at the designated time (Figure 1) [23].
Descriptive data
The mean age (SD) of respondents was 24.25 (5.682), ranging from 18 to 40; 83.3% were below 30 years old. Mean (SD) time span of disease duration was 13.71 (6.203) years, ranging from 5 to 25 years. Furthermore, the mean body mass index (BMI) (SD) was 23.50 (3.050), indicating desirable average weight of selected patients; 66.7% of patients had BMI lower than 25 kg/m2, while 33.3% of patients had BMI ranging from 25 to 29.9 kg/m2 (classified into grade I obesity category according to Garrow classification) [24]. Fitzpatrick’s skin type II (66.7% of the patients) was prevailing in our study, while there were no patients with Fitzpatrick’s skin type IV (Table 1). The lowest UV index value our patients experienced was 6, and the highest was 9. The mean UV index (calculated for each patient, for all 14 days of HT) ranged from 6.714 to 9.
Table 1
Demographic and clinical characteristics of the patients included in the sample
Changes in SCORAD and EASI indices, DLQI and SPS scores in three times
The mean initial SCORAD at T1 was 25.91. There was a statistically significant reduction in SCORAD index after 2 weeks of HT (mean SCORAD at T2 = 15.13), as well as 3 months after HT (mean SCORAD index at T3 = 19.30). Additionally, 1 patient experienced complete clearance at T2. SCORAD index fell down by 40% in T2 comparing to the baseline (p < 0.001, r = 0.87, Z = –4.29), and SCORAD remained decreased by 31.1% at T3 comparing to baseline values (p < 0.001, Z = –4.294, r = 0.88). The mean EASI score at T1 was 20.92. Like SCORAD index lowering, EASI score reduced significantly by 49% and 31% at T2 and T3. It was noted that 2 patients reached zero EASI score at both second and third appointment (T2 and T3).
The changes in SCORAD and EASI indices were accompanied by the changes in the DLQI score. The mean DLQI value at T1 was 11.42. We observed a statistically significant reduction in DLQI score at both T2 and T3 comparing to T1 value. The mean DLQI score at T2 and T3 was 6.92 and 8.29, respectively. The results revealed a statistically significant decrease in DLQI score by 31.57% (Z = –4.320, p < 0.001, r = 0.88) at T3 in contrast to the baseline value.
Finally, the outcomes showed a statistically significant reduction in SPS scores at three times. The mean baseline SPS score was 1.42, while it dropped to mean 1.00 at T3 (Tables 2, 3).
Table 2
SCORAD indices and EASI scores measured at three times
Table 3
DLQI and SPS values measured at three times
Discussion
AD has an appreciable influence on the quality of life, thus it is of crucial importance to control and bring down the severity of the disease as much as possible. We tried to compare the outcomes of our study with the results obtained from the scarce resources of studies assessing the effectiveness of HT.
Patients included in the study had a range of SCORAD index from 7 to 62, suggesting that they belong to the following clinical forms of AD: SCORAD lower than 25 – mild clinical form, SCORAD from 25 to 50 – moderate clinical form, and SCORAD over 50 – severe clinical form [25]. The mean baseline SCORAD value was 25.91, and remained significantly decreased at T2 and T3. One of the patients experienced complete clearance at T2, and the same patient had 1 point SCORAD index due to sleeping disturbances at T3. The SCORAD index value was lower by 40% and 31.1% at T2 and T3, respectively, comparing to the value at T1. These results suggest that individual 2-week HT does not have only short-acting effect, but favourable effects in clearing the skin changes for a longer period of time. A study conducted by Autio et al. showed even more exceptional results, stating that SCORAD index was reduced by 70% immediately after 2-week HT and remained decreased by 45% after 3 months of the therapy. Furthermore, the mentioned study showed no statistical significance of mean SCORAD indices between the patients who received 2 weeks of HT comparing to those who received 3 weeks of HT [26]. Therefore, it is considered that 2-week HT is optimal as 3-week HT did not provide additional benefits. On the other hand, a study conducted by Karppinen et al. and Kudish et al. showed results that are fairly similar to ours. In the first study, patients attended 2-week HT resulting in PO-SCORAD decreasing from 30.6 by 19.5 units and 10.0 units at T2 and T3, respectively [27]. Additionally, the latter study was assessing climatotherapy on children with AD showing a persisting low SCORAD index with an overall average improvement of 71.3% 3 months after the therapy [28].
There are fairly more studies examining HT effects in patients with psoriasis using PASI (Psoriasis Area and Severity Index) score in order to evaluate skin changes/disease severity after the therapy. A study conducted by Karppinen et al. showed that mean SAPASI was reduced by 73% after 2-week HT, and it remained reduced by 46.3% 3 months after HT [27]. As PASI and SCORAD are not comparable with each other mainly because SCORAD includes subjective components along with the visible signs, we calculated EASI score. Our study showed a slighter reduction in EASI score at T2 (reduced by 49%) and T3 (reduced by 31%), comparing to the results from the mentioned psoriatic study, but it was still statistically significant.
We used standardized DLQI questionnaire to measure the impact of HT on the QoL. There was a statistically significant reduction in DLQI scores both at T2 and T3, comparing to the baseline. Special interest of our study was assessment of possibility of HT in improving the QoL in the long run. Surprisingly, our results showed a reduction in DLQI score by 31.57% (p < 0.001) at T3 comparing to T1 value. These results imply long-term benefits of HT in improving the QoL in patients with AD. Similar outcomes, regarding the long-lasting improvement in the QoL are in accordance with the study conducted by Karppinen et al. in 2015, when the authors assessed the effects of HT using DLQI questionnaire both in patients with psoriasis and AD. The long-lasting improvement in the QoL 3 months after 2-week HT was not achieved among the patients with psoriasis. Contrary to that, they did prove long-term (3 months after 2-week HT) improvement in QoL in patients with AD [27]. We believe that these results are fairly encouraging and may be a turning point for posing HT on a higher level of the treatment ladder, especially in the countries with plenty of sunshine hours [29]. However, there is a considerable demand for more scientific research studies assessing the long-term effects of HT on the QoL in patients with AD.
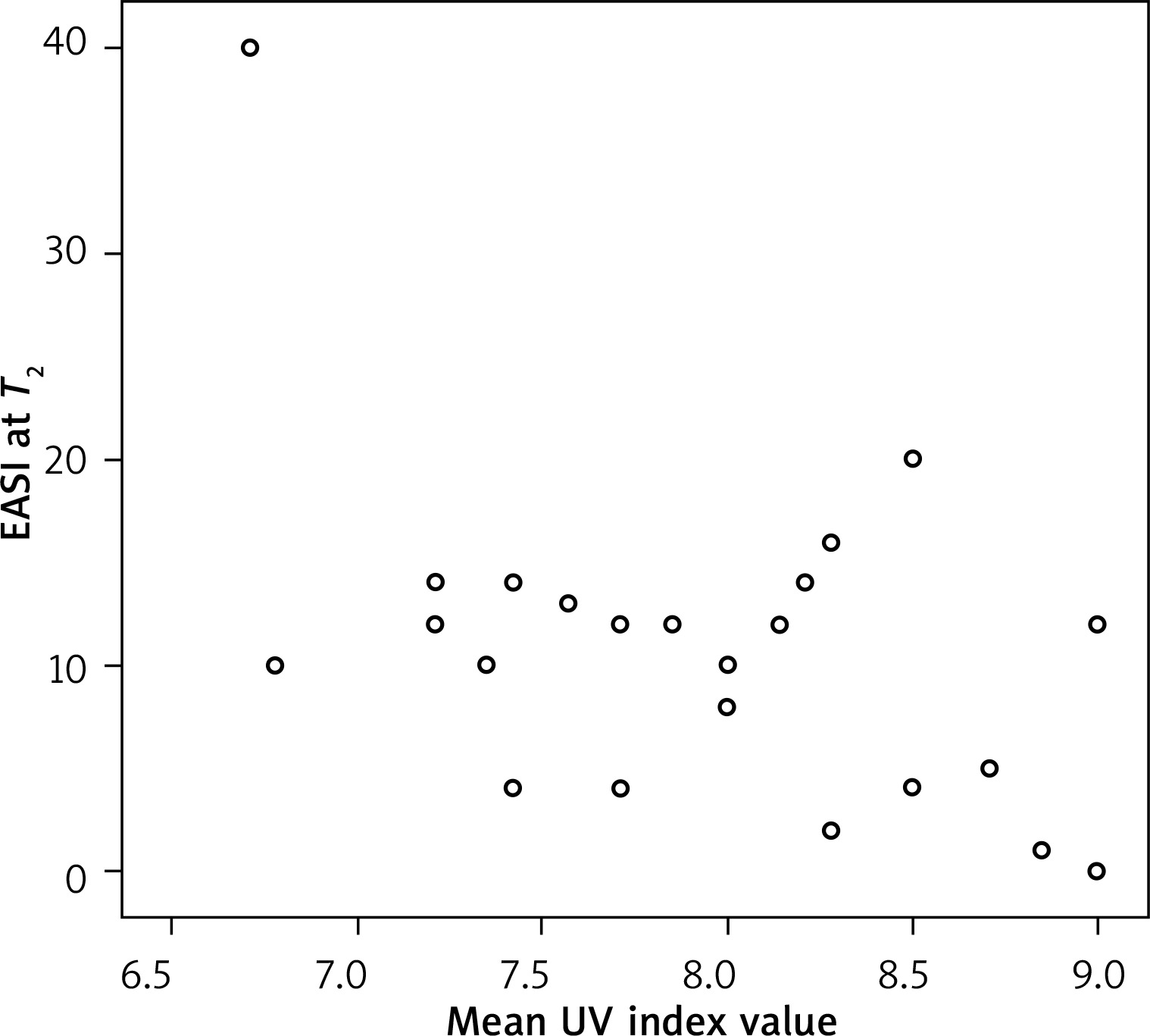
Using different statistical tools, we tried to find a correlation between patients’ age, comorbidities, duration of AD or BMI and DLQI/SCORAD/EASI change. No such correlation was confirmed. On the other hand, we did find a strongly negative correlation of individual EAS I scores both at T2 and T3 with mean individual UV index (r = –58; p = 0.002). This suggests that the higher the UV index, the lower the EASI score change (Figure 2).
Figure 2
Correlation between the mean UV index of each patient and the change in EASI score 14 days after HT
The main limitation of the study could be the absence of peer support due to individuality of the HT program. HT or climatotherapy usually includes meeting peers, mutual support among peers, practicing healthy lifestyle such as physical activity, psychological support and social well-being. All in all, natural UV therapy even in its individual form has been proved to have very satisfying long-acting effects among patients with atopic eczema, making it worthy of pursuing. Moreover, studies imply that HT has a persistent effect regarding the QoL. As HT is not recognized as a standard treatment modality among health care officials in many countries including ours, we believe that more studies with solid results would be helpful to include HT in the national health care policy programs for patients with atopic eczema. As mentioned, Montenegro is a country with plenty of sunshine hours, therefore organizing even group heliotherapies would not be excessively money-consuming.
Conclusions
The impressive and satisfying clinical and epidemiological results obtained in the presented study could be explained by following reasons: the favourable mechanism of action of UV lights on inflammatory dermatoses through its immediate and delayed effects, avoidance of well-known triggering and provocative factors during HT, as well as safe exposure to UV lights [30]. The HT model has been evaluated predominantly on patients with psoriasis, resulting in lack of firm data about its effects on the patients with AD. So far, studies have shown even more satisfying results regarding the QoL in patients with AD comparing to the patients suffering from psoriasis [27]. These results should encourage both physicians and patients to use this treatment option, as well as researchers to seek firm confirmation of the immediate and delayed effects of HT.